UT Southwestern Medical Center has more than 30 years of experience and innovation in the surgical treatment of aneurysms, often offering technologies and treatments before they become available at other centers.
With 24/7 availability, we serve as a major referral center for second opinions and complex cases in the Dallas-Fort Worth area and the entire state of Texas. Our cerebrovascular team routinely cares for patients from Oklahoma, New Mexico, Arkansas, and Louisiana.
Our neurosurgeons, neurologists, and radiologists are fellowship-trained in the surgical and endovascular treatment of aneurysms, allowing our team to offer a well-rounded approach for whatever level of treatment is needed.
Finding the Right Treatment for Each Patient
UT Southwestern neurosurgeons offer expertise in both surgical techniques and minimally invasive endovascular approaches to treating aneurysms.
Each procedure has different strengths. Specialists at UT Southwestern work with patients to determine which solution will achieve the most effective results for them. The technique we use depends on each patient’s unique situation – along with the size, shape, and location of the brain aneurysm.
Minimally Invasive Procedures for Brain Aneurysm
Minimally invasive options do not require an incision in the skull, which lowers the risk of complications and reduces the length of hospital stay. UT Southwestern was among the first neurosurgical departments to train its neurosurgeons in endovascular techniques (1995). Our neuroradiology team was instrumental in designing one of the first endovascular devices that is still used today, and, as a result, our surgeons have years of experience in using a variety of these techniques.
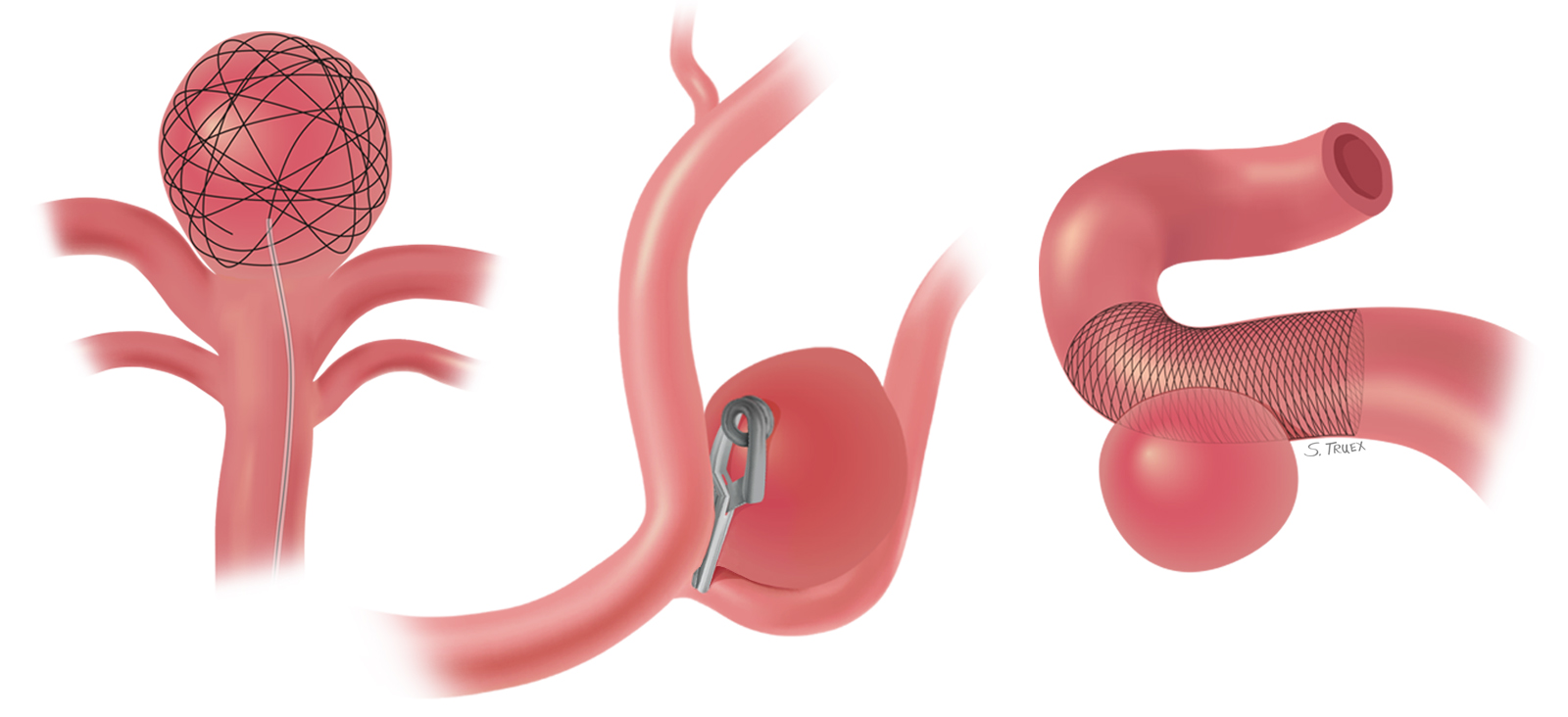
Coiling
Endovascular coiling uses a catheter to reach the aneurysm. The catheter is inserted into an artery of the groin or arm and threaded into the artery containing the aneurysm. One or more coils are then placed into the aneurysm through the catheter.
These coils are flexible and conform to the shape of the aneurysm, and they slow blood flow and cause the blood to clot. A scar will then form across the aneurysm neck, which effectively heals the aneurysm and helps prevent future rupture. The coils are made of platinum, so they're visible on an X-ray. An MRI can be performed when these coils are present.
When performing a coiling procedure, we might use additional devices, such as a stent, to help keep the coils in place. Stent-assisted coiling involves placing a mesh stent in the blood vessel adjacent to the aneurysm as scaffolding to keep the coil within the aneurysm. Patients will need to be able to take blood-thinning medications if a stent is placed.
Flow Diversion
Flow diversion can be used for a select group of aneurysms. Typically, these are larger lesions (more than 10 mm) with a wider opening. In this procedure, very specialized stents made of a braided mesh are placed in the parent blood vessel to divert blood flow away from the aneurysm. These stents are similar to a traditional stent but are more tightly woven – think of a stocking (flow diversion) versus chicken wire (standard stent). These stents have the potential to reconstruct the wall of the artery and restore natural blood circulation.
Flow diversion removes the need to enter the aneurysm during surgery, but it requires the use of blood-thinning medications for a longer period of time than traditional stent devices.
Surgical Treatments for Brain Aneurysm
People with certain risk factors, such as those whose aneurysms are more likely to recur with coiling or those who are not able to take blood thinners, might benefit from surgical solutions. UT Southwestern neurosurgeons offer expertise in surgical techniques such as clipping and bypass. This skill is becoming rarer because of the popularity of endovascular therapy and is found at only the most experienced medical centers.
Clipping
In this procedure, a neurosurgeon opens the skull and places a small metal clip at the base of the aneurysm to tie off the bulging section of the artery. This clip eliminates the danger of a rupture by taking the pressure off the weakened area of the blood vessel.
For an unruptured aneurysm, a patient typically spends three to five days in the hospital after clipping. The stay is longer after surgery for a ruptured aneurysm.
Bypass Surgery
Extracranial-to-intracranial bypass surgery is used to treat complex, unclippable brain aneurysms. Similar to bypass surgeries for the heart, this procedure uses a vein from the leg or an artery from the arm or scalp grafted to bypass blood flow around the artery that is affected by the aneurysm. This delicate procedure is performed at only a few major U.S. medical centers. UT Southwestern neurosurgeons are highly experienced in this procedure, which is also used to treat conditions such as moyamoya syndrome and skull base tumors.
Recovery and Rehabilitation
After treatment, patients recover in our dedicated neurointensive care unit. The length of the stay depends in part on the treatment received.
The Neuro-ICU at UT Southwestern’s Zale Lipshy Pavilion – William P. Clements Jr. University Hospital has the largest number of specialists in neurointensive care in North Texas. It’s staffed by a team of physicians, nurses, patient care technicians, respiratory therapists, and ancillary staff – who together provide specialized care to manage all aspects of life-threatening cerebrovascular disorders.
We also offer neurorehabilitation for those who need physical, occupational, or speech therapy.