

Search for opportunities to participate in a clinical research study.
Facial Paralysis of the Eyes
New Patient Appointment or 214-645-8300
One of the most important areas to protect – and always a priority in treatment – is the eye on the paralyzed side. Patients may have difficulties or find it impossible to close the eye due to paralysis of the orbicularis oculi muscle that surrounds the eye.
This may result in exposure of the cornea, causing significant corneal irritation characterized by redness, irritation, and a feeling of a foreign body. This condition, known as exposure keratopathy, is usually worse in the morning.
If left untreated this condition may develop into ulcerations, scarring, and even blindness. In addition to difficulty closing the eye, facial nerve paralysis often causes dry eye due to decreased tearing.

A patient with right paralytic lagophthalmos, attempting to close her eyes before treatment.

A patient's eyes after treatment.
Passive Strategies for Treating a Paralyzed Eye
Continuous lubrication and covering of the eye at night
The first step, regardless of any planned surgeries, is to keep the eye lubricated all day and also covered at night. This is done with a combination of eye drops, ointment, and occasionally a moisture chamber, which is eyewear that protects the eye, especially during sleep by maintaining moisture around the eye.
In cases of Bell's palsy, when many patients will improve on their own or the situation will resolve itself, lubrication treatment may be the only kind needed. Surgical solutions are needed in cases when incomplete resolution or no recovery is expected.
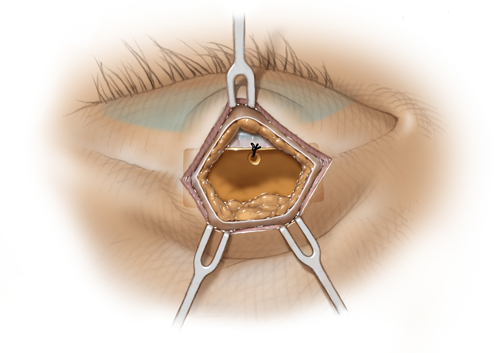
Weighting of the upper eyelid with gold or platinum weights
Weight placement and fixation to the levator aponeurosis superior to the tarsal plate, a technique that hides the goldweight.
Among the more common surgical solutions to treat an inability to completely close the lower eyelid is insertion of a weight in the upper eyelid. This may be a platinum or gold weight. The principle behind this treatment is to use gravity during sleep to obtain protective closure of the upper eyelid.
These weights will often remain in the upper eyelid, but they may be removed or downsized if partial recovery is observed.
Weight placement and fixation to the levator aponeurosis superior to the tarsal plate, a technique that hides the goldweight.
Lower eyelid surgery
Patients often develop a situation in which a lower eyelid droops below the one on the uninjured side and more of the white of the eye is seen. The lower eyelid also is turned inside out.
Several procedures may be performed based on the severity and laxity of the lower eyelid. Most involve repositioning the lower eyelid in addition to providing further support.
Lifting the brow
The majority of patients suffering from facial paralysis experience some sagging of the forehead and brow. Patients generally exhibit drooping of the eyebrow compared to the other side and they cannot raise the brow, causing severe asymmetry and deformity.
Surgery may be used to raise the brow. The surgery is specifically tailored to the patient and may involve lifting the brow behind the hairline, or lifting the brow directly, which is more common and often more effective.
Dynamic Strategies for Treating a Paralyzed Eye
Dynamic restoration means the return of motion to the paralyzed side. The dynamic restoration of the eye area refers to the ability to close the eye voluntarily and possibly develop some degree of blink reflex.
Not all patients are candidates for reconstruction of the eye area. Critical factors to consider include the:
- Reason for the paralysis
- Degree of injury to the nerves
- Amount of viable muscle that remains intact
- Timing of reconstruction
Reconstruction procedures may include nerve graftings or nerve transfers. Results vary based on the type of injury, the elapsed time between the injury and the time of seeking treatment, and the condition of the muscles and nerves at the time of evaluation.
Related Conditions and Treatments


We’re one of the world’s top academic medical centers, with a unique legacy of innovation in patient care and scientific discovery.

MedBlog






Results: 3 Locations
Ophthalmology
at UT Southwestern Monty and Tex Moncrief Medical Center at Fort Worth 600 South Main Street, 1st Floor, Suite 1.500Fort Worth, Texas 76104 817-429-3050 Directions to Ophthalmology at UT Southwestern Monty and Tex Moncrief Medical Center at Fort Worth, Fort Worth Parking Info for Ophthalmology
Ophthalmology Clinic
at James W. Aston Ambulatory Care Center 5303 Harry Hines Blvd., 6th FloorDallas, Texas 75390 214-645-2020 Directions to Ophthalmology Clinic at James W. Aston Ambulatory Care Center, Dallas Parking Info for Ophthalmology Clinic
Plastic Surgery Clinic - Facial Paralysis
at Outpatient Building 1801 Inwood Road, 5th FloorDallas, Texas 75390 214-645-2353 Directions to Plastic Surgery Clinic - Facial Paralysis at Outpatient Building, Dallas Parking Info for Plastic Surgery Clinic - Facial Paralysis