A century ago, the father of modern neurosurgery Dr. Harvey Cushing helped us understand the function of the pituitary gland – the pea-sized gland that sits on a bony cavity at the base of the brain and helps regulate functions such as blood pressure, growth, and body temperature.
Dr. Cushing pioneered surgical approaches to reach and remove pituitary adenomas (non-cancerous tumors) from the tiny-but-mighty gland, and his technique, which ultimately required opening the skull, remained the gold standard until the last few decades.
Modern neurosurgery is much less invasive. For most patients, we can remove a pituitary tumor by accessing it through the nose. Endoscopic skull-base tumor resection allows for faster recovery, reduced pain and discomfort, and fewer potential complications. UT Southwestern’s specialized pituitary adenoma team performs two to five of these procedures each week.
Pituitary adenomas are considered brain tumors, but they are almost exclusively benign (non-cancerous). Left untreated, however, the tumors can grow and cause life-altering symptoms such as vision changes, low blood pressure, fatigue, menstrual irregularities, and diminished sex drive. While no specific cause for pituitary adenomas has been identified, they account for 10% of all brain tumors and occur more frequently in women.
Skull-base tumor treatment requires the combined expertise of otolaryngologists (ear, nose and throat specialists), such as myself, and a neurosurgeon. We also work closely with our colleagues in endocrinology, neurology, ophthalmology, and radiation oncology to ensure all of our patients’ needs are met from the moment symptoms arise.
Discovering a pituitary adenoma
Despite its modest size, the pituitary gland plays an important role in nearly every part of your body’s function. It’s often referred to as the master gland because it directs other glands to release essential hormones.
So, when a tumor begins to grow on your pituitary gland it can create a range of symptoms, which differ based on whether the tumor is pressing on nearby structures or if it is secreting a hormone. (In some cases, the tumor may be asymptomatic.)
Pressure from a growing adenoma can cause headaches or, if it’s pressing on the optic nerve it may cause double or blurred vision, even temporary blindness. If the adenoma pushes on the pituitary gland itself, symptoms can include low blood pressure, fatigue, weakness, symptoms of hypothyroidism, menstrual irregularities, and a decreased sex drive.
If the tumor secretes hormones, the symptoms depend on which hormones are being released. The most common hormones related to pituitary adenomas include:

- Adrenocorticotropic hormone (ACTH): These tumors stimulate the production of cortisol, leading to Cushing’s disease (named after Dr. Cushing). Symptoms may include rapid weight gain, excessive sweating, easy bruising, high blood pressure, high blood sugar, absent or missed menstrual periods, impotence, and reduced libido.
- Growth hormone: Symptoms may include enlarged hands, feet, nose, lips, or ears; heart problems; joint pain; and increased body hair.
- Prolactin: Overproduction of this hormone can cause a decrease in normal levels of sex hormones, leading to irregular or absent periods, milky breast discharge, decreased libido, and erectile dysfunction.
- Thyroid-stimulating hormone (TSH): Overproduction of this hormone can cause weight loss, rapid heart rate, hair loss, fatigue, weakness, and excessive sweating.
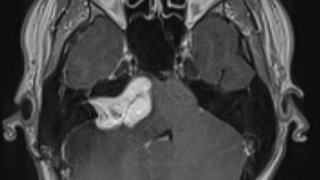
Pituitary adenomas are usually diagnosed with an MRI scan, though large tumors can sometimes be seen on a CT scan. The tumor also can be diagnosed through blood tests for hormone levels.
Some pituitary adenomas don’t cause symptoms and if they’re discovered incidentally on an MRI or CT scan, we may watch them closely without recommending removal. Other pituitary adenomas may be treated with medications or targeted radiation therapy (Gamma Knife).
However, if the tumor is growing, compressing important structures, or secreting hormones, it most likely will require surgery to remove it.
Related reading: What women need to know about common benign brain tumors
Endoscopic pituitary adenoma surgery
Removing a small or average-sized pituitary tumor requires a team of experts and takes place in several stages: approach, removal, and reconstruction. According to the American Association of Neurological Surgeons, more than half of pituitary adenomas are diagnosed when they are 5mm or smaller in diameter, or about the size of pencil eraser.
After you are put under general anesthesia, an otolaryngologist will access the tumor by inserting two small, lighted tubes (endoscopes) into the nostrils and through the sphenoid sinus, a hollow space in skull behind the nasal passages and below the brain.
Once we reach the pituitary gland, the surgeons will work in tandem – the otolaryngologist often operates the endoscope to illuminate the adenoma and provide visibility while the neurosurgeon uses crafted instruments to see around corners in the narrow areas of the skull base to resect, or cut out, the tumor.
Then, we remove the tumor through the nose and make sure the healthy tissue in your nasal structures and sinuses is as undisturbed as possible. This sequential surgery takes about 3 to 4 hours. The surgeons will place temporary packing material in your sinuses to hold the healing tissue in place. We will remove it approximately a week after surgery.
Tumors that cannot be completely removed endoscopically will sometimes require additional treatment like focused radiation.
Targeting tumors with precision radiation
Brain tumors that cannot be completely removed endoscopically will sometimes require additional treatment like focused radiation using the advanced Gamma Knife technology.
Recovering from pituitary adenoma surgery
Patients typically stay in the hospital three or four days after surgery, so we can ensure the pituitary gland resumes normal functioning. Most patients do not need strong medications to control the pain after surgery. However, the sinuses may be sore or uncomfortable due to the temporary nasal packing.
Recovery from the minimally invasive procedure is usually excellent, and you can return to normal activities and work relatively soon after leaving the hospital. In some cases, there may be spinal leakage during surgery, which means you may need to take it easy a little longer to allow that to heal fully.
You’ll likely need to return at least once a year for an MRI to make sure the pituitary adenoma has not returned. If the tumor caused hormonal deficiencies, you may need ongoing care and supplements from our endocrinology team.
UT Southwestern’s Comprehensive Skull Base Program treats a large volume of pituitary adenomas each year – a condition seen only rarely in most centers – so our team is able to provide patients with customized, multidisciplinary care using the latest technology available.
Endoscopic skull-base surgery is a huge leap forward from Dr. Cushing’s pioneering work in the early 1900s. Today’s patients can live long, healthy lives after pituitary adenoma removal – with a fast and safe recovery following treatment.
To visit with a pituitary adenoma expert, call 214-645-8300 or request an appointment online.