Partnering with Our Patients
Having patients informed about and actively engaged in discussing treatment options is key to our approach to care. When determining appropriate care plans, our physicians consider:
- The size and growth rate of the acoustic neuroma
- The patient’s overall health
- Signs and symptoms the patient is experiencing
Treatment options that our UT Southwestern Acoustic Neuroma Program offers include:
Observation
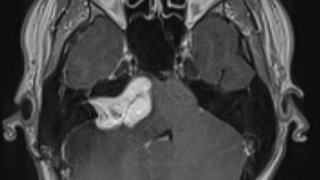
Some patients, particularly those with smaller, slow-growing tumors, don’t require immediate treatment. We may recommend monitoring these cases. With this watch-and-wait approach, our physicians use advanced imaging to look for changes that could signal the need for additional treatment.
Radiosurgery
Gamma Knife radiosurgery is a noninvasive, precisely focused dose of radiation that targets a tumor with the goal of stopping its growth. Key advantages of radiosurgery for patients include minimal recovery time and preserving quality of life. It is performed on an outpatient basis. Many of our patients have no symptoms immediately after having this procedure.
Microsurgical Resection
Microsurgical resection techniques let us safely remove the tumor while preserving facial nerve function whenever possible. This option is best for patients with larger or more complex tumors, as well as those with smaller tumors where preserving hearing is possible.